
This is a malignant disorder (or cancer) of myeloid precursor cells, called also myeloblasts. Normally myeloblasts mature into red blood cells, platelets, or the white cell types called monocytes and granulocytes. Cell formation is abnormal in this type of leukaemia and myeloblasts accumulate in the bone marrow. Sometimes they go also into blood and occasionally into other organs, commonly into spleen, or liver.
These abnormal leukaemic myeloblasts very quickly build up in the bone marrow, preventing normal cell development. As a result there are not enough normal white blood cells, red blood cells, or platelets. The lack of white cells predisposes to infections; insufficient red cells causes anaemia, with symptoms of shortness of breath and tiredness. Low platelets may predispose to easy bleeding and bruising.
There are different subtypes of AML. Some, such as acute promyelocytic leukaemia can be distinguished by looking at the bone marrow cells under the microscope. For other subtypes of AML special testing is required, such as testing for changes in the genes of affected cells. Acute promyelocytic leukaemia has a specific therapy which includes administration of a very potent form of vitamin A – tretinoin, together with chemotherapy. For other forms of AML, initial therapy is usually similar and then is tailored by specific subtype.

The reason why most people develop acute myeloid leukaemia is unknown. Exposure to certain chemicals such as benzene or to radiation may contribute to development of leukaemia. This includes people previously treated with chemotherapy or radiotherapy. Acute myeloid leukaemia is also slightly more common in smokers. It is not a contagious disease. Although chromosomes of leukaemic cells can be abnormal, leukaemia does not get passed directly from parents to their children.
Acute myeloid leukaemia can occur at any age but the risk increases with age; it is therefore most common in elderly people. In general younger patients have higher curative success rates, but exact predictions of success of therapy are very complex.
Treatment of acute myeloid leukaemia is a complex and lengthy procedure. In younger patients the aim is to achieve cure. In elderly people or people with significant other health problems this may not be possible and the aim is to prolong meaningful life. Therapy has two main components; supportive care, which includes providing red cell and platelet transfusions and prompt treatment of infections and secondly the systemic anti-cancer therapy. This includes administration of chemotherapy sometimes combined with targeted anti-leukaemic therapy or immunotherapy including allogeneic bone marrow transplantation.
There are other uncommon types of leukaemia:
-
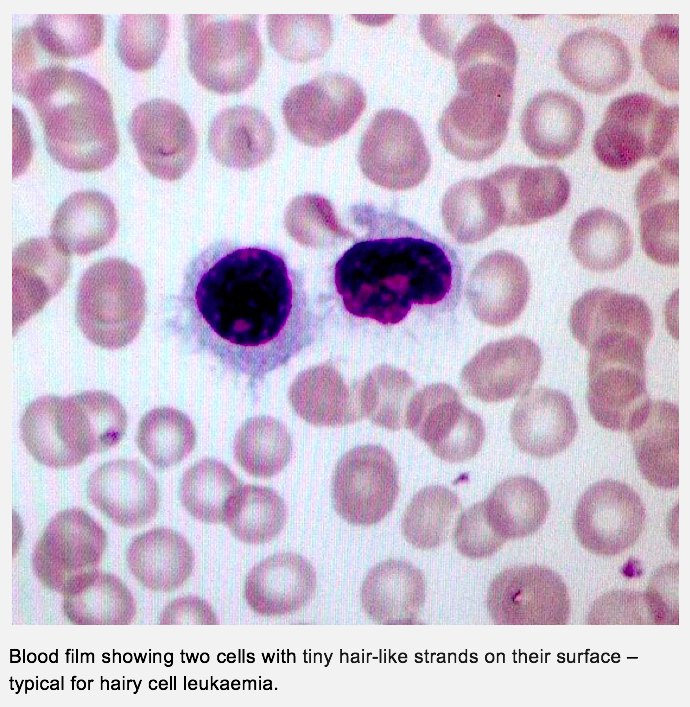
- Hairy cell leukaemia (HCL) – this is a rare type of leukaemia that affects lymphoid precursor cells. When examined under the microscope the leukaemic cells appear to have tiny hair-like strands on their surface. This leukaemia develops very slowly and often enlarges the spleen. Hairy cell leukaemia sometimes may not need any treatment. If treatment is needed, chemotherapy given into the vein is used: cladribine (2-chloro-deoxy adenosine) or pentostatin (deoxycoformycin) are good and long-lasting control of hairy cell leukaemia.
-
- Large granular lymphocytic leukaemia (LGL leukaemia) – this is a rare type of leukaemia that affects lymphocytes. Blood and bone marrow examination shows enlarged lymphocytes with granules. There are two main forms, an aggressive type that is very rare and may developed quickly and a chronic, slowly developing form. Patients with the aggressive type may develop enlargement of the liver, spleen or lymph nodes. As this leukaemia is extremely rare, there is no standard generally agreed treatment but intensive chemotherapy is recommended, sometimes followed by bone marrow (haematopoietic stem cell transplantation). However, most patients affected with LGL leukaemia will have a chronic, slowly developing form. They may experience no problems. Low red cell count (anaemia) or low neutrophil count (neutropenia) are common. Sometimes patients develop an enlarged spleen. Many patients with this chronic form do not require any therapy. Large granular lymphocytic leukaemia develops more often in patients with rheumatoid arthritis. In this context the leukaemia responds to treatment with immunosuppression. Intravenous chemotherapy may sometimes be useful.
-
- Plasma cell leukaemia (PCL) – this is a very rare type of leukaemia. It is very similar to a blood cancer called multiple myeloma. The affected cells in both plasma cell leukaemia and multiple myeloma are related to lymphocytes and are called plasma cells, which normally make antibodies. Signs and symptoms are similar to those in myeloma and this link leads to more information.
For more information about leukaemia try following link: Blood Cancer UK