
The stage measures how widely has a lymphoma spread around the body. The Ann-Arbor staging system is the most commonly used and has four stages. Stages I and II are referred to as early stage and III and IV are considered advanced stages.
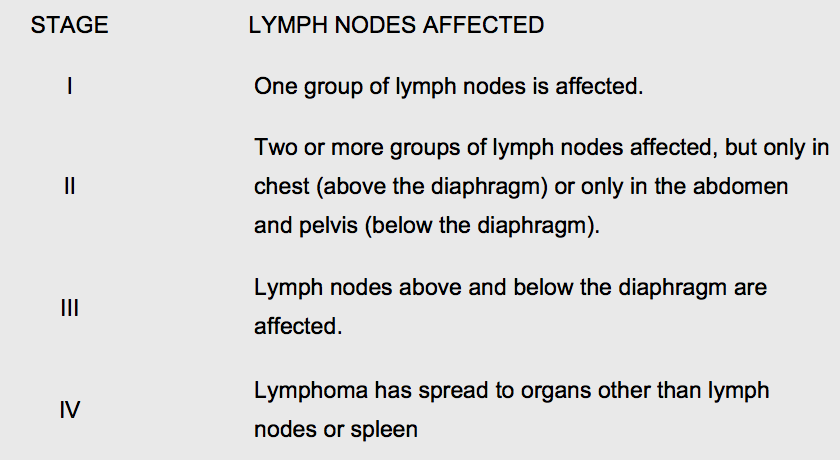
In addition to this the system uses the letter A for patients without significant night sweats, significant weight loss or lymphoma-associated fever, and the letter B for patient with these symptoms. The letter S is used for lymphoma that has spread to the spleen and the letter E if it has spread outside lymph nodes or spleen.
The majority of patients with lymphoma are diagnosed with non-Hodgkin lymphoma. Like Hodgkin lymphoma this is not a single disease but a large group of very different cancers. Some of them are slow growing, indolent and may not even require any treatment. Other types can be very aggressive, fast growing and make patients unwell rapidly. Some types are well known to respond favourably to treatment and some are not. The subtypes are characterised by their appearance under the microscope, the pattern of proteins within the membranes of lymphoma cells and by changes in different genes. New types of rare lymphoma are still being described.
Most non-Hodgkin lymphomas are related to lymphocytes called B cells and are therefore called B cell lymphomas. Some lymphomas are related to T cells and rarely lymphomas can be related to other types of lymphocytes.
Common B cell lymphomas are:
-
- Diffuse large B cell lymphoma – this is the most common rapidly growing (aggressive) lymphoma. It can affect people of any age but is more common in older individuals. Treatment includes chemotherapy infused into the vein, often together with monoclonal antibodies (immunotherapy). Stem cell or bone marrow transplantation may sometimes be useful, particularly if the lymphoma relapses after initial treatment. Although aggressive lymphomas present with severe symptoms and complications, most patients will be cured with immunotherapy and chemotherapy.
-
- Marginal zone lymphoma – slow growing (indolent) lymphomas that affect older people. There are three subtypes of this lymphoma. Mucosa-associated lymphoid tissue (MALT) lymphoma affects lymphoid tissue in stomach, bowels and endocrine glands. Sometimes a microorganism is responsible for causing MALT lymphoma. In these cases, treatment sometimes does not require chemotherapy but antibiotics may suffice. Nodal marginal zone lymphoma affects lymph nodes and splenic marginal zone lymphoma affects the spleen. Marginal zone lymphomas sometimes do not require therapy. If treatment is necessary it may be with localised radiotherapy or chemotherapy in combination with monoclonal antibodies.
-
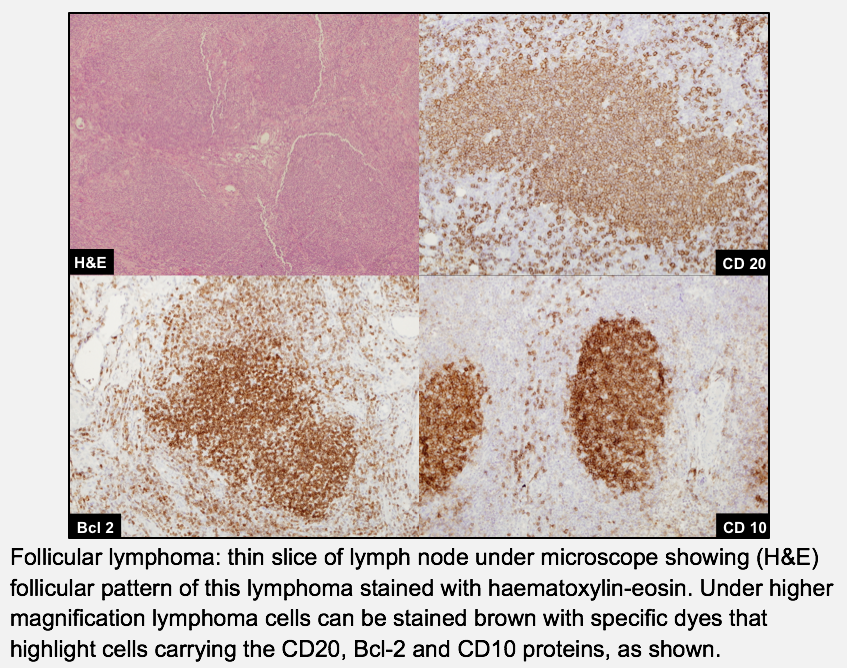
- Follicular lymphoma – this is the most common type of slow growing (indolent) lymphoma. Follicle means a small sac, gland or an aggregate of cells and this type of lymphoma is called follicular because of the appearance of the affected lymph nodes under the microscope. Under magnification there are apparent aggregates or clumps of abnormal cells. (see figure below).
-
- Follicular lymphoma is more common in people aged over 50 years, but it can occur in people of any age. It usually grows slowly but occasionally it is known to change into fast growing diffuse large B cell lymphoma. This change is called transformation.
-
- Treatment of follicular lymphoma depends on its stage, the problems that it causes, but also on each individual patient’s fitness to cope with the side effects of chemotherapy and radiotherapy. Sometimes, if patients have no or only few medical complaints no treatment is needed. In stage I, radiotherapy to the affected lymph nodes offers a good treatment option with few side effects and can be suitable for frail patients. More advanced stages require chemotherapy given together with immunotherapy (monoclonal antibodies) to control the disease. Stem cell (bone marrow) transplantation is sometimes used. Chemotherapy can provide very good control of this lymphoma in most patients. However, the only treatment that can cure advanced follicular lymphoma is transplantation using stem cells from a different person (allogeneic transplantation). Because this treatment is complex and associated with many side effects, it is typically offered to fit patients who have relapsed several times.
-
- Mantle cell lymphoma – this type of lymphoma originates from the mantle zone of lymph nodes. Mantle cell lymphoma has the appearance of a slow growing lymphoma under the microscope, however it usually behaves as a relatively aggressive disease. It sometimes spreads to the bowel or bone marrow and is treated with chemotherapy given together with immunotherapy (monoclonal antibodies). Young and fit patients should also undergo Stem cell (bone marrow) transplantation to achieve a long-lasting remission.
-
- Burkitt lymphoma – this is a relatively rare type of lymphoma, which exists in many forms. It is very aggressive and grows very fast. Burkitt lymphoma tends to spread outside of lymph nodes. Sometimes Burkitt lymphoma presents as a medical emergency. Despite its aggressive presentation, Burkitt lymphoma can be cured in many patients with prompt treatment including inpatient, intensive chemotherapy and supportive care.
The most common T-cell lymphomas are:
-
- Peripheral T-cell lymphoma – this is not a single lymphoma but a group of many relatively rare T-cell lymphomas. The most common subtype in this group is peripheral lymphoma not otherwise specified (PTCL - NOS) and it is itself made of many different subtypes of peripheral T-cell lymphoma. These are more common in people over the age of 60 and they usually grow rapidly. Therapy is with chemotherapy given into the vein and Stem cell (bone marrow) transplantation is recommended in young and fit patients.
-
- Angioimmunoblastic lymphoma – this rare lymphoma is usually fast growing (aggressive) and it is more common in older individuals. Sometimes patients with this type of lymphoma develop itchy skin rashes or joint pains. It is also sometimes associated with other blood diseases in which the immune system attacks its own body such as autoimmune haemolytic anaemia. Treatment includes administration of corticosteroids and chemotherapy. Young and fit patients should be treated with Stem cell (bone marrow) transplantation.
For more information about leukaemia try following link:
Lymphoma association
Leukemia and lymphoma society